Last Updated on March 18, 2026 by Admin
Bursiter is the inflammation of a small, fluid‑filled sac called a bursa (plural: bursae), which acts as a cushion between bones and surrounding soft tissues like muscles and tendons. These bursae help joints move smoothly by reducing friction during motion.
Bursiter — more widely known in medical literature as bursitis — can be painful, limiting, and frightening when it first appears. This article breaks down everything you need to know: what bursiter is, why it happens, how clinicians diagnose it, the most effective treatments (from home remedies to medical interventions), and practical prevention strategies you can start using today. The goal is to deliver expert, reassuring guidance that helps readers feel confident, informed, and empowered to take action.
RELATED: Holisticke: Embrace Wellness, Balance & Mind-Body Harmony
What is Bursiter?
Bursiter is the inflammation of a small, fluid-filled sac called a bursa (bursae) that cushions bones, tendons, and muscles around joints. These bursae act as low-friction shock absorbers — helping tissues glide smoothly during movement. When a bursa becomes irritated or swollen, the result can be localized pain, warmth, and restricted range of motion. Mayo Clinic.
Bursiter is not a single-location problem: it can affect many bursae across the body, producing symptoms that depend on the bursa’s location. Understanding that bursiter is fundamentally an inflammatory process helps guide both conservative self-care and targeted clinical interventions.
How Bursiter differs from other joint conditions
Bursiter differs from tendinitis (tendinopathy) and arthritis in where and how the pain originates. Tendinitis is inflammation or degeneration of tendons (the strong cords that attach muscle to bone), whereas arthritis primarily affects joint cartilage and the joint capsule. Bursiter is localized to the bursa — a distinct anatomical structure — and often produces surface swelling that moves differently from joint pain. This difference is important for diagnosis and for selecting the right treatment approach.
Clinically, bursiter pain tends to worsen with direct pressure or specific movements that compress the bursa (for example, kneeling for prepatellar bursiter or lifting for subacromial bursiter). In contrast, arthritic pain often has a deeper joint ache and stiffness, and tendon injuries typically produce pain with tendon loading. These distinctions guide both self-care and clinical evaluation.
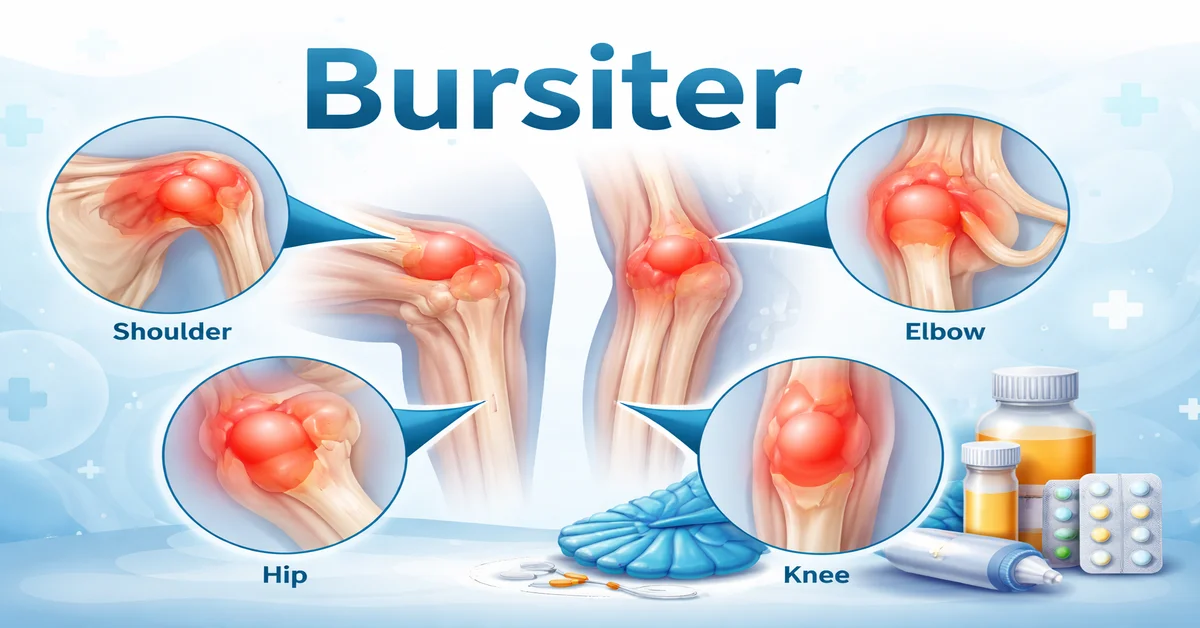
Common joints affected (shoulders, elbows, hips, knees)
The most commonly affected bursae are found around the shoulder (subacromial/subdeltoid), elbow (olecranon), hip (trochanteric), and knee (prepatellar & pes anserine). Other important sites include the Achilles region (retrocalcaneal bursitis), iliopsoas bursa (hip/groin pain), and ischial bursa (weaver’s bottom). The symptoms and treatment approach depend on the exact location.
Knowing the typical locations helps patients and clinicians quickly suspect bursiter when localized swelling and pain match these common patterns — speeding up relief and recovery.
Causes of Bursiter
Repetitive motion and overuse
Repeated movements or sustained activities that stress a specific joint are among the most common triggers of bursiter. Examples include frequent overhead motions in tennis or painting (shoulder bursiter), constant kneeling in gardening or floor work (knee bursiter), and repetitive elbow pressure in plumbing or leaning (olecranon bursiter). Overuse causes microtrauma and irritation that gradually inflames the bursa.
Occupational and athletic populations are particularly at risk — but anyone who suddenly increases repetitive activity can develop bursiter. Addressing the movement patterns that caused the problem is often central to long-term recovery.
Prolonged pressure on joints
Sustained direct pressure on a bursa — for example, kneeling for long periods or resting the elbows on hard surfaces — can compress and irritate the bursa, provoking inflammation. Protective padding (kneepads, elbow pads) and small ergonomic changes can dramatically reduce this pressure and prevent recurrence.
For workers in trades and sportspeople, modifying task mechanics or using protective gear often reduces flare-ups faster than medication alone.
Injury and trauma
A direct blow to a joint (a fall onto the knee or elbow) can damage the bursal lining and cause rapid fluid accumulation and swelling. Traumatic bursiter may present with immediate, visible puffiness and pain, and while some cases settle with conservative care, others require aspiration or medical assessment to rule out bleeding or infection.
Infection (Septic Bursiter)
Septic bursiter occurs when bacteria invade the bursa, typically after a small skin break over a bursa (scrape, insect bite, or puncture). Septic bursiter often produces marked redness, warmth, fever, and increased pain. Prompt diagnosis and antibiotic treatment are essential; empiric coverage often includes agents active against skin organisms such as Staphylococcus aureus, including MRSA-active options when local prevalence suggests it. Aspiration of bursal fluid for culture guides definitive therapy. NCBI Bookshelf – StatPearls.
Underlying health conditions (arthritis, gout, diabetes)
Systemic conditions can predispose to bursiter. People with rheumatoid arthritis are prone to inflammatory bursae; gout can cause urate crystal deposition and secondary bursal inflammation; diabetes can increase susceptibility to infection and slower healing. Managing these underlying conditions reduces risk and helps recovery.
Age-related factors
With age, cumulative joint wear and changes in tissue resilience make bursae more vulnerable to inflammation. Older adults who remain active can still get bursiter — and age often alters the balance between conservative care and when to escalate treatment. Regular conditioning, flexibility work, and ergonomics remain powerful prevention tools at any age.
Symptoms of Bursiter
Pain types – sharp vs dull
Bursiter presents with pain that can be sharp (during movement or when pressure is applied) or dull and aching at rest. Pain often increases with specific joint use — for example, lifting the arm for shoulder bursiter or kneeling for knee bursiter — which helps clinicians distinguish bursiter from other causes. Mentioning the movement or posture that provokes your pain is clinically useful.
Swelling and fluid accumulation
Inflamed bursae often accumulate excess fluid, producing visible swelling or a noticeable “puffy” area over the joint. In some bursae (like the olecranon or prepatellar), the swelling is obvious; in deeper bursae (subacromial), swelling may be less visible but still cause pain and restricted motion. Imaging or aspiration can confirm fluid.
Stiffness and limited range of motion
Inflammation and swelling reduce the joint’s range of motion. This stiffness can make daily tasks — reaching, climbing stairs, or kneeling — painful and limited. Early movement guided by a therapist often prevents stiffness from becoming chronic.
Warmth, redness, and signs of infection
Warm, red skin over the bursa — often accompanied by fever — raises concern for septic bursiter. This presentation warrants urgent evaluation, aspiration, and possible antibiotics. Don’t ignore systemic signs (fever, spreading redness) — these are red flags that need medical attention.
Chronic vs acute bursiter symptoms
Acute bursiter typically follows a clear trigger — sudden overuse or injury — and improves with rest and short-term care. Chronic bursiter results from recurrent irritation or untreated triggers and may require a multi-modal approach (therapy + activity change + targeted injections). Chronic pain often benefits most from a combination of strengthening, stretching, and ergonomic correction.
Diagnosing Bursiter
Physical examination and medical history
Diagnosis starts with a detailed medical history and physical exam: clinicians check for localized tenderness, swelling, warmth, and movements that provoke pain. Asking about occupation, recent activity changes, and systemic symptoms (fever, joint disease) helps determine the next steps. The physical exam will often localize the affected bursa and exclude obvious alternatives.
Imaging techniques (X-ray, ultrasound, MRI)
X-rays are useful to rule out fractures or bone spurs but don’t show bursae directly. Ultrasound is excellent for detecting bursal fluid and guiding aspiration or injections, while MRI offers detailed views for complex or deep-seated bursae and helps evaluate surrounding tendons and joint structures. Choosing the right imaging depends on clinical suspicion and response to initial care.
Bursal fluid aspiration and lab tests
When infection is suspected or when swelling is significant and persistent, clinicians may aspirate the bursa (withdraw fluid with a needle). Fluid analysis (cell counts, Gram stain, culture) differentiates septic from aseptic bursiter and guides antibiotic selection. Aspiration can also relieve pressure and pain.
Differential diagnosis – tendonitis, arthritis, frozen shoulder
Other common causes of joint pain — tendinitis, arthritis (rheumatoid or osteoarthritis), and frozen shoulder (adhesive capsulitis) — can mimic bursiter. Careful exam, imaging, and sometimes trials of therapy clarify the diagnosis. For instance, tendon pain is provoked by active loading of the tendon, whereas bursiter is more movement/pressure sensitive.
Treatment Options for Bursiter
Rest and activity modification
Initial treatment typically begins with rest and avoiding activities that provoke symptoms. Short-term removal of the offending motion allows inflammation to subside and prevents further damage. For workers and athletes, this may include task modification or temporary role adjustments. Conservative measures often achieve full recovery.
Ice therapy and RICE method
Applying cold packs (ice wrapped in cloth) for 15–20 minutes several times daily reduces swelling and numbs pain. The classic RICE approach (Rest, Ice, Compression, Elevation) remains useful for many superficial bursae and is an accessible first step for home care.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Over-the-counter NSAIDs (ibuprofen, naproxen) reduce pain and inflammation. They are effective for many cases but should be used per label and clinician guidance, particularly for those with gastrointestinal or cardiovascular risk factors. Topical anti-inflammatories can be an alternative to systemic therapy for some patients.
Corticosteroid injections
For persistent or severe bursiter, a corticosteroid injection directly into the bursa can provide powerful anti-inflammatory relief lasting weeks to months. Ultrasound guidance improves injection accuracy. Injections are an excellent option to break a pain cycle while a patient begins rehabilitation exercises.
Physical therapy and exercises
Physical therapy focuses on restoring motion, strengthening surrounding muscles, and correcting body mechanics that contributed to the problem. A targeted rehabilitation program reduces recurrence risk and builds long-term resilience. Examples include rotator cuff strengthening for shoulder bursiter or quadriceps/hip abductor work for trochanteric bursiter.
Aspiration of fluid and antibiotics for septic bursiter
When an infection is suspected, aspiration plus culture guides antibiotic selection. Empiric antibiotics often cover skin flora including MRSA in areas with high prevalence; severe infections may require IV antibiotics and inpatient care. Managing septic bursiter promptly avoids deeper spread of infection.
Surgery in severe cases
Surgical bursectomy (removal of the inflamed bursa) is rare but considered for chronic, refractory cases that fail conservative and interventional treatments. Most patients respond well to non-surgical care, making surgery an infrequent final option.
Home Remedies and Lifestyle Management
Natural pain relief options
Gentle topical therapies (cold packs, arnica gels, menthol creams) and anti-inflammatory supplements (e.g., omega-3 fatty acids) can supplement medical care. While evidence varies, many patients find meaningful symptom relief from combined conservative measures. Always discuss supplements with your clinician, especially if you take medications.
Exercise routines to prevent flare-ups
Low-impact strengthening and stretching routines support joint stability and reduce bursiter recurrence. Focused programs for the shoulder, hip, or knee — prescribed or reviewed by a physical therapist — ensure safe progression and correct form. Consistency is the strongest predictor of success.
Ergonomic practices and protective gear
Use kneepads, elbow pads, or cushioned supports when occupational tasks demand prolonged pressure on joints. Ergonomic adjustments at work — raising/lowering surfaces, using long-handled tools, and alternating tasks — significantly reduce stress on bursae and lower flare-up rates.
Diet and anti-inflammatory foods
Eating a balanced diet rich in anti-inflammatory foods (colorful vegetables, fatty fish, whole grains) supports general recovery and joint health. Avoiding excessive processed foods and sugars helps reduce systemic inflammation and may aid healing. Diet is an adjunct, not a substitute, for targeted medical care.
Preventing Bursiter
Proper posture and body mechanics
Good posture and proper lifting mechanics reduce unnecessary compression and friction across bursae. Movement coaching, ergonomic assessments, and mindful technique while exercising or working can prevent many cases of bursiter. Small adjustments often produce large benefits.
Strengthening muscles around joints
Strong muscles around a joint absorb forces that otherwise load the bursa. Regular resistance training — guided by a professional if needed — protects joints and stabilizes movement patterns that would otherwise provoke inflammation.
Reducing repetitive strain at work or sports
Rotate tasks, take micro-breaks, and cross-train to avoid repetitive stress. Employers and coaches who plan for rotation and recovery reduce injury risk and improve long-term performance and comfort. Simple scheduling and equipment changes can prevent chronic problems.
Maintaining a healthy weight
Excess body weight increases the mechanical load on weight-bearing bursae (hips, knees). Even modest weight loss reduces joint stress, lowers inflammation, and decreases the likelihood of bursiter recurrence. Weight management is a powerful, long-term prevention strategy.
RELATED: Senaven: Supplement Review, Benefits, Ingredients & Safety
Frequently Asked Questions (FAQs) About Bursiter
Can bursiter heal on its own?
Yes — many cases of bursiter, especially mild or acute overuse cases, resolve with rest, ice, and activity modification within a few days to weeks. Conservative care and early movement safely restore function in most people.
How long does recovery take?
Recovery varies: minor cases may improve within 1–3 weeks; more severe or chronic bursiter can take months, especially if causative activities continue. Combining rest, therapy, and targeted interventions accelerates healing.
Can bursiter become chronic?
Yes. If the underlying cause (repetitive motion, pressure, or poor mechanics) isn’t corrected, bursiter can recur and become chronic. Strengthening, ergonomic changes, and medical management reduce this risk.
When should I see a doctor?
Seek immediate care if you notice fever, spreading redness, or severe pain — signs that infection may be present. Otherwise, see your clinician if symptoms persist beyond a week of self-care, limit daily activities, or keep recurring. Timely assessment prevents complications.
Summary
Bursiter is common, often treatable, and frequently preventable. Early identification of the cause (overuse, pressure, injury, or infection) and prompt, appropriate care produce the best outcomes. Conservative strategies — rest, RICE, NSAIDs, and targeted physical therapy — resolve most cases; infections require antibiotics and urgent care.
H3: Steps to manage and prevent bursiter
Start with activity modification, ice, and gentle movement. Use ergonomic tools and protective padding, strengthen surrounding muscles, and seek professional advice when pain persists. For suspected infection or unrelenting symptoms, pursue medical evaluation promptly.
H3: Encouragement for proactive joint care
With knowledge and small, consistent changes, bursiter rarely needs drastic measures. Invest in proper technique, balanced training, and early care — your joints will thank you with lasting comfort and improved performance.